Blackie Laminitis Case
This is an acute laminitis case that was initially painful and exhibiting the typical founder stance on December 16 2012. No known cause but a mild colic episode had occurred 3 days prior. I was able to perform venograms on what I would consider Day one of laminitis. These plain film radiographs and venograms create a baseline in which to compare follow up venograms. This allows assesment of the mechanical therapy applied and severity of compromise in the days to follow. Venograms 5 days later show moderate compromise already. Consider the amount of compromise present while treated with mechanics. Unloading the Deep flexor tendon, its forces applied to the dorsal lamellar zone and sole directly below tip of coffin bone via raising the palmar angle.
There is no measurable displacement of the bone but significant change has occured within the vascular network as early as five days. Some financial constraints existed and it was decided to wait 30 days and repeat venograms to evaluate if the mechanics applied would be enough. I warned the client at this point that a deep flexor tenotomy may need to be performed as this rapid progression is very concerning. Ideally a repeat venogram in another 4-7 days would have been best but finances limited to a 30 day check. Knowing what I know now about this case I would have cut tendons on day five and never looked back. Below is the Day one venogram on the left compared to the Day five Venograms on the right side. Focus your eyes on the circuflex artery, terminal papillae and the vasculature directly below the tip of coffin bone. Moderate compression and diplacement of these vessels five days into the syndrome. Remember that no measurable rotation, increase in h/l zones, loss of sole depth has occured.
After applying the modified ultimates on day one the horse began to make a clinical improvement noted by moving around in stall better and better appetite. He no longer rocked back to make turns. This is important to consider as clinical signs alone are not good indicators of how the case is going. The horse will lie to you when comes to laminitis.
 |
| Right Front venogram comparson Day one to Day five |
 |
| Left Front Venogram comparsion Day one to Day five. |
 |
| Day 5 |
 |
| Day five |
Below are venograms that are 30 days post laminitis of the left front. Note the circumflex is several milimeters above the tip of the coffin bone and no papillae are present. I again recommended deep flexor tenotomy as the modified ultimates are not providing enough mechanical relief, through unloading the force of the deep flexor. The tenotomy abolishes all forces applied to the bone to hoof attachments and solar corium directly below tip of coffin bone. Finances prohibited the Owner from going the surgical route and horse was actually improving with regard to pain and we decided to wait another thirty days.
 |
| 30 Days Post. The Circumflex artery is displaced several mm above the tip of the coffin bone and the solar vasculature is tightly compressed below the tip of the coffin bone. |
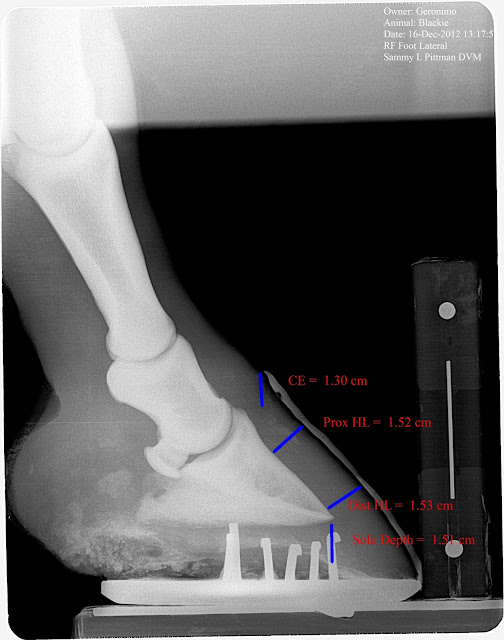
Below are 60 day post radiographs. Note the increased C/E distance, diverging H/L zones (rotation),and loss of sole depth, especially on the Left. No growth is noted on examination of the dorsal hoof wall and about 1/4 in at the heels is noted. Just to recap, we have no measurable displacement of the bone until 60 days into the syndrome but significant vascular changes on day five that continues to fail despite mechanical therapy. If you are waiting to diagnose laminitis based on rotation you are 60 days late in this case.
 |
| 60 day post insult radiograph. Note changes in ce, hl zones and sole depth. |
 |
60 Days post initial insult. Note diverging hl zones (some may call rotation) increased in ce and comparable decrease in sole depth.
|
Below are comparative venograms of the left front. On the left is day one and on the right is 90 days after intial insult. Note the greatly altered circumflex architecture and the tip of the coffin bone is visualized below the solar vessels. Moderate thickening of the dorsal sublamellar zone and significant accumalation of contrast as the dorsal coronary band that is likely secondary to a septic process that is brewing. Horse still has not grown any sole or dorsal hoof wall in 90 days. Note the scallop like loss of bone that occurs just above the tip caused by displacement of the terminal papillae and circumflex artery. I can only assume the combination of local hydraulic pressure and possibly the redirected papillae in this area are to blame for this unique change in the shape. At this stage in the game many irreversible changes have occurred that will likely prevent this horse from returning to a previous level of competition.
 |
| 90 days post comparison |
 |
| 90 days post comparison . The right foot has suffered less but prominent and significant change/damage has occurred in the area of the circumflex artery and terminal papillae. |
 |
| Left front Post tenotomy and derotation. |
 |
| Right Front post tenotomy and derotation. |
At the 90 day examination I advised the client that surgery was the only option for treatment and this late in the game I could only offer a guarded prognosis for any return to previous level of performance. The owner opted to donate the horse for a learning seminar. On March 22, 2012 a little over 90 days post initial insult a eager bunch of vet students and farriers performed venograms, applied derotation shoes and performed deep flexor tenotomies. In the days following the horse is moving much better. I will post followup radiographs in 30 days to evaluate the progress. I do feel recovery is still very likely. Ideally performing the tenotomy prior to irreversible damage and bone change would result in a better outcome.
In conclusion I would like to re iterate the important points:
1) In hindsight a deep flexor tenotomy should have been performed on day five or very shortly after.
2) Improvement with regards to pain and movement are not good indicators of success in laminitis.
3) Radiographic measurements alone, early in the syndrome, may change very little if any and a venogram may be the only information alluding to the nature of the insult.
4) Aggressive early mechanical therapy did relieve a lot of pain but did not provide enough unloading of the Deep digital flexor to aid in unloading of the vascular supply and further unloading via deep flexor tenotomy would have likely given a better outcome if performed earlier.
Stay tuned!
LOBO Laminitis Case.
Welcome again, This is a case of acute laminitis that we were called to look at late on the evening of May 29, 2011. History of colic episodes the previous couple of days but now not wanting to stand and when does stand has typical laminitis stance. Upon examination normal foot conformation no ridges but large bounding pulses noted in all four feet. Placed in Nanric modified ultimates which raise the palmar angle 18-20 degrees and Lobo immediately began to show signs of comfort with licking of lips, less distress and standing up squarely on fronts. He was still reluctant to move in a normal fashion. Baseline radiographs are taken on this evening and have soft tissue parameters within normal range. This is where many hoof care professionals are confused as no signs of bone displacement or rotation has occurred, but it is still very important to support this foot mechanincally with wedging to unload effects of the deep digital flexor tendon as the vascular compromise has likely began. The idea that if there is no rotation it is no laminitis/founder does not hold true. This will also show how important radiographs on day 1 of exam are so valuable when compared to the next visit 5 days later. A baseline venogram was not performed as finances where limited at this point.


We returned to visit Lobo five days later and find he has been laying down the biggest part of the time which is probably to his advantage as all load is off feet and better circulation is allowed. Radiographs on this day show significant soft tissue parameter changes with large increases in CE, H/L zones and decrease in sole depth. Palpable ledge is noted on both fronts at the coronary band that is consistent with a sinker. We performed a venogram at this point at no charge to client to further increase our knowledge of this case. The changes in soft tissue parameters indicative of a moderate sinker are confirmed with the venogram with no perfusion at the coronary waterfall, face of coffin bone and sole under tip of p3. Note even in this severe case the heels remain great perfusion. The unloaded view is taken with the limb being held up which gives us an idea of what the perfusion may be while laying down with tendon and foot completely unloaded and some indication of what it would look like with a tenotomy to completely release any action on the coffin bone.
The venogram is performed in the modified ultimate which unloads the flexor tendon by 60 percent. This also serves as a means to evaluate a certain therapeutic package. If your plan is to restore healthy blood supply then you should be able to prove that the package is going to do that via the venogram. This venogram suggest that the modified ultimate will not be enough to restore proper blood supply and that further mechanical release via deep digital flexor tenotomy would likely improve the situation as the sharp border of the coffin bone is cutting through the sensitive solar corium and its vital blood supply. Several methods to prevent the bone from displacing are practiced but few have been confirmed and followed with serial venograms and radiographs to prove that they are unloading the circumflex artery. The heart bar shoe is a positive force applied to the frog in order to antagonize the displacement of the coffin bone, but think about the tissue between the rigid heart bar and the coffin bone. The solar corium with its blood supply that makes the horny sole that we can see and touch. Obviously it has helped many cases but I think a further study as to it's affects on foot perfusion in a laminitis scenerio via serial venograms and radiographs is warranted. Below is the radiographs and venograms from the second visit 5 days later. I will also post a normal venogram for comparison.
 |
| NORMAL VENOGRAM FOR COMPARISON TO LOBO'S |





We were unable to perform suggested derotation and tenotomy as financial constraints did exist. Owner opted to give Lobo more time as he was laying down which is protecting the vital blood supply. Contact was made with owner approximately 6 weeks after second visit and Lobo was not improving and he was ready to euthanize and I offered to take Lobo to further his treatment and if not able to be successful I would humanely euthanize if needed. Lobo was transported to IEPVS and new radiographs and venograms performed. Notable hoof wall growth had occured and was surprisingly very close to even from toe to heel. Moderate improvement in venograms in areas of the coronary band, face of p3 and tip of p3. Considerable displacement of the circumflex still exist and very severe compression of vascular bed under apex of p3 is still present. Note the changes in the soft tissue parameters on the lateral films. Note the lucent zone that indicates the level of separation of the horn/lamellar zone. Despite improvement of venogram, more mechanical release in the area of the circumflex and solar vascular bed is need and derotational shoeing and tenotomy was performed. Note the red line is the trim line and guide for shoe placement. The shoe is a 5 degree rail shoe with a trailer welded in to prevent the toe from tipping up after DDF tenotomy. The shoe is placed at zero palmar angle with a minimum of 20 mm space below p3 and the 5 degree helps prevent painful subluxation of the coffin joint. This shoe is atraumatically applied with adhesive and nylon strips. Two part silicon rubber is used to prop shoe up and apply caudal solar weight distribution.




 |
| POST TENOTOMY RADIOGRAPH |
 |
| TENOTOMY RAIL SHOE, POST TENOTOMY RADIOGRAPH |
Lobo has went from laying down 90 percent of the time to standing 90 percent of the time. Attitude and appetite have greatly improved. The plan is to recheck venogram and lateral radiographs in 2-3 weeks after tenotomy. I will gladly post those so we can all learn from this case. With the amount of bone remodeling that has already occurred to the fragile thin rim of coffin bone it is less likely we will have as good of a response as we would have if derotational shoeing and tenotomy where performed in the important window of opportunity at the second visit. However, I do expect a great improvement in the hoof growth and patient comfort. The amount of bone resorption will be what prevents Lobo from returning to a previous level of perfomance. We will have to wait and see.
******Update on this case***********As of January 2015 this horse is ridden regularly with no signs of lameness and barely a noticeable bump at the site of tendon surgery.
Stay tuned for more exciting podiatry cases!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!







{kind=link}





















No comments:
Post a Comment