Saturday, May 26, 2012
Sunday, April 8, 2012

Please call 918.235.1529 or email iepvs11@gmail.com to register as seating will be limited.
Monday, April 2, 2012
Hello out there in the horse world. We are off to a busy start with many new podiatry cases, vaccinations, floats and yearly wellness exams.
I wanted to post a couple of recent cases that drive home two very important points regarding therapeutic shoeing. Both cases are in rocker shoes. One because of crushed heels and poor foot mass and the second due to a low grade navicular bone lesion. Both cases where started in rocker shoes and have been sound. However after another farriers reset without radiographic guidance as per request of the Owner to help reduce cost both horses went lame. I ruled out any likelihood of close nails and horses are exhibiting only low grade lameness.
After radiographs where performed and measurements taken the shoe and trim were slightly modified. Below are the differences in pre and post shoe measurements that seemed significant to me and could likely be the reason that both cases where not as sound as previously.
Take some time and compare and contrast each radiograph for each case.
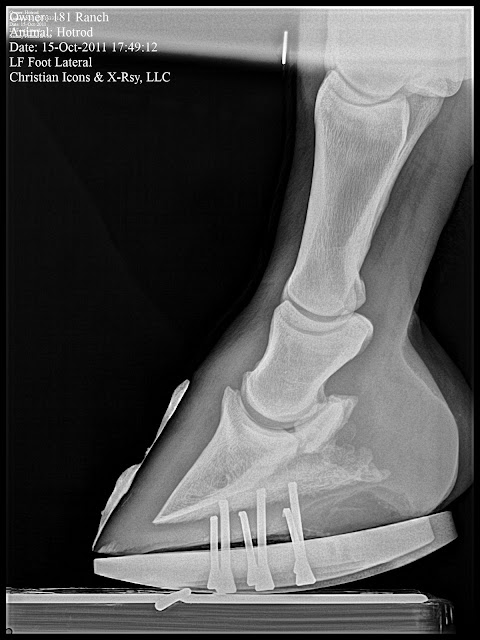
Note the major differences in digital alignment, palmar angle, toe lever, tendon surface angle and suspensory ligament of navicular bone distance. The changes noted radiographically help explain why this horse would be lame. The mechanics governed by the trim, shape and placement of the rocker alter loads inside the foot. With the PA much lower a higher degree of tension can be expected within the deep digital flexor unit and more hyperextension applied to the coffin and pastern joint. A recent paper suggest that for every degree change in PA, pressure on the navicular bone changes 4%. We changed load on the navicular apparatus by around 24 %. Note the distance measured from the navicular bone to the origin of the suspensory ligament of the navicular bone. This changed 6mm and may also be another reason for increased comfort with higher mechanics. The last important aspect is the toe lever, measured from COA to where the shoe would leave the ground. This is the affective lever arm that gives the ground advantage to apply force to the flexor tendon apparatus. This number was greatly changed and subsequent reduction in force applied to DDFT is achieved.
This horse has mild navicular bone changes and has responded very nicely to the rocker shoe approach. The increased PA and reduced digital break over has this horse back in the show ring. This one has baffled me as after the farrier reset horse was just slightly off in soft footing and traveled almost normal on hard surface. On initial exam the PA and shoe placement appeared to be in good shape. However when in soft footing the horse would tend towards a rocking back approach, which I assumed to increase pressure on DDFT and navicular apparatus.
I wanted to post a couple of recent cases that drive home two very important points regarding therapeutic shoeing. Both cases are in rocker shoes. One because of crushed heels and poor foot mass and the second due to a low grade navicular bone lesion. Both cases where started in rocker shoes and have been sound. However after another farriers reset without radiographic guidance as per request of the Owner to help reduce cost both horses went lame. I ruled out any likelihood of close nails and horses are exhibiting only low grade lameness.
After radiographs where performed and measurements taken the shoe and trim were slightly modified. Below are the differences in pre and post shoe measurements that seemed significant to me and could likely be the reason that both cases where not as sound as previously.
Take some time and compare and contrast each radiograph for each case.
 |
| Farriers reset |
 |
| Post radiograph trim and shoe |
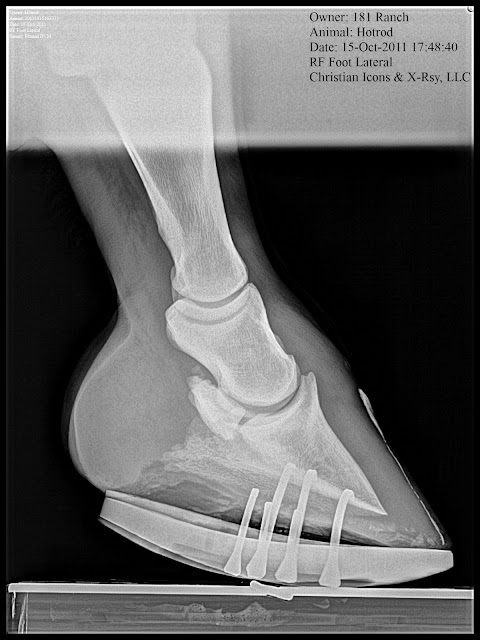
Note the major differences in digital alignment, palmar angle, toe lever, tendon surface angle and suspensory ligament of navicular bone distance. The changes noted radiographically help explain why this horse would be lame. The mechanics governed by the trim, shape and placement of the rocker alter loads inside the foot. With the PA much lower a higher degree of tension can be expected within the deep digital flexor unit and more hyperextension applied to the coffin and pastern joint. A recent paper suggest that for every degree change in PA, pressure on the navicular bone changes 4%. We changed load on the navicular apparatus by around 24 %. Note the distance measured from the navicular bone to the origin of the suspensory ligament of the navicular bone. This changed 6mm and may also be another reason for increased comfort with higher mechanics. The last important aspect is the toe lever, measured from COA to where the shoe would leave the ground. This is the affective lever arm that gives the ground advantage to apply force to the flexor tendon apparatus. This number was greatly changed and subsequent reduction in force applied to DDFT is achieved.
 |
| Farriers reset |
 |
| Post radiograph re trim and shoe |
The measurable differences are a shortened toe lever and a much lower PA, however the Suspensory ligament distance and the TSA remained very similar despite the lower PA. This is very confusing and I will continue to try to wrap my head around this one. I think the key here was reshaping the rocker to place directly under center of articulation versus slightly behind and modification of the trim in the same manner. I feel with the belly/rocker to far back this forced a higher than needed PA and created a scenerio that allowed for rapid sinking of the heel in soft footing. Jogged sound in hard and soft footing after changes where made.
Take home message:
1) Not all rocker shoes are the same.
2) Radiographs are a valuable tool in many difficult cases.
I feel that if radiographs where available, for the farriers that reset these shoes, this could have been avoided as there are obvious mechanical differences noted in the radiographs. Many times have I pulled a shoe and modified it after seeing the radiograph and I am thankful for that advantage.
Do not blame the anything but the mechanics! Do you really know what they are?
Note to Owners: Yes radiographs can be the difference between your horse being sound or lame.
Note to farriers and veterinarians: Do not blame the rocker shoe, heartbar, egg bar, or whatever device applied without critical evaluation of the mechanics that the foot is subjected to. If something did not work try to figure out why. Through serial radiographic evaluation of every foot problem one can develop an enormous amount of information and detail that can allow such great success.
All the best,
Sammy
Monday, January 23, 2012
NANRIC Blog: Slideshow - Rockering a Rail Shoe
NANRIC Blog: Slideshow - Rockering a Rail Shoe: This slideshow of photos from Dr. Redden illustrates how to rocker a rail shoe.
Great slideshow of Dr. Redden Rockering a 4pt rail shoe which is used to treat many common fool ailments such as: chronic laminitis, navicular syndrome and thin soles.
Have a great week.
Wednesday, January 11, 2012
Update On Lobo the Laminitis Case.
Previous Post on Lobo. Click on the link to the left for the first post. Lobo is responding very well to the Tenotomy performed back in July. He continues to grow hoof wall at an even rate toe to heel and continues to add good dense sole. I would not consider success if those are not occurring. In evaluation of your laminitis treatment if you are still growing more heel than toe then you are not effectively addressing the mechanical problem. ie more tendon release is needed either with an increase in Palmar angle or likely a tenotomy.
I placed Lobo in Rocker rails as he began to have upright pasterns indicating the need for more mechanics (increase in PA), and due to the affects of the tenotomy which removes most of the load on the dorsal lamellar attachments and solar corium at the apex of the coffin bone but increases load through heels. The only load is distributed through the bone column through the palmar (back) aspect of the hoof which over time will add some heel crush. This is best addressed with the rocker or the buttress trim.
I (and Lobo) liked the increase in palmar angle but I was not fond of how he could rock back in soft footing. This being due to the lengthening of the deep digital tendon post tenotomy. I moved him into an aluminum buttress with a five degree rail, which accomplished my goal of a higher palmar angle and ability to remove all crushed heel and load to widest part of frog. The buttress shoe trim involves creating a positive palmar angle by trimming from the toe back with the rasp tipped at a 5-8 degrees. This is continued approxiametly the wings of the coffin bone ideally. The heels are then taken at an angle parallel to the palmar angle to the widest part of the frog. The buttress wedge bar is made of 1/2 by 1 inch aluminum bent in to a U - shape to fit the width of the heels. Forge a wedge shape to fit your trim. Grinding or hammering a recess in the bar for the frog will necessary in most cases. I really like this approach for my post tenotomy cases when added mechanics are needed to maintain good digital alignment. This will occur in more severe cases when vascular and bone damage occur secondary to laminitis insult that was either not appropriately addressed in a timely fashion or so severe that any mechanics would not have changed things sucha as in severe sinker cases. Lobo did not receive the needed tenotomy until 6 wks post laminitis and the initial insult was severe creating compromise at the circumflex. This is noted in the venogram obviously but also in the shape of the tip of the coffin bone. You can see flipped up circumflex starting to remodel around the apex.
 Maintained in tenotomy rail then a four point trim. This is when we noted a need for more mechanics noted by upright pasterns.
Maintained in tenotomy rail then a four point trim. This is when we noted a need for more mechanics noted by upright pasterns.

 Initially placed in Rocker Rail to increase PA and removed crushed heels.
Initially placed in Rocker Rail to increase PA and removed crushed heels.







 This is the Left series which shows similar improvement as the right. Good remodelling around the circumflex b ut poor solar and terminal papillae. I feel that even with even toe to heel growth and good sole depth that unless solar papillae return with more healing and regeneration time then any chance of a performace career will be limited.
This is the Left series which shows similar improvement as the right. Good remodelling around the circumflex b ut poor solar and terminal papillae. I feel that even with even toe to heel growth and good sole depth that unless solar papillae return with more healing and regeneration time then any chance of a performace career will be limited.
Points to remember: Evaluation of the vascular supply is paramount to determine success of the device you are applying. Success should not only be measured by comfort of the patient but I cannot claim success without even toe to heel growth and addition of 7-10mm of sole depth every 30 days. If this is not happening one must rethink their approach. Note we did not have a natural increase in Palmar angle we created is due to upright pasterns. The upright pasterns can be secondary to continued low grade bone pain or even some heel pain. Achieving better digital alignment allows load be directed through the middle of the foot in the direction that the first phalanx is pointing.
Lobo is now getting 4-6 hours of paddock turnout after five months of stall confinement with the first three in firm wraps over tenotomy site to prevent excessive scarring and a tenotomy rail shoe to prevent toe from flipping up or undue strain on tenotomy site in soft stall bedding.
Please comment, email (iepvs11@gmail.com) or call (9182351529) if you have any questions.
I placed Lobo in Rocker rails as he began to have upright pasterns indicating the need for more mechanics (increase in PA), and due to the affects of the tenotomy which removes most of the load on the dorsal lamellar attachments and solar corium at the apex of the coffin bone but increases load through heels. The only load is distributed through the bone column through the palmar (back) aspect of the hoof which over time will add some heel crush. This is best addressed with the rocker or the buttress trim.
I (and Lobo) liked the increase in palmar angle but I was not fond of how he could rock back in soft footing. This being due to the lengthening of the deep digital tendon post tenotomy. I moved him into an aluminum buttress with a five degree rail, which accomplished my goal of a higher palmar angle and ability to remove all crushed heel and load to widest part of frog. The buttress shoe trim involves creating a positive palmar angle by trimming from the toe back with the rasp tipped at a 5-8 degrees. This is continued approxiametly the wings of the coffin bone ideally. The heels are then taken at an angle parallel to the palmar angle to the widest part of the frog. The buttress wedge bar is made of 1/2 by 1 inch aluminum bent in to a U - shape to fit the width of the heels. Forge a wedge shape to fit your trim. Grinding or hammering a recess in the bar for the frog will necessary in most cases. I really like this approach for my post tenotomy cases when added mechanics are needed to maintain good digital alignment. This will occur in more severe cases when vascular and bone damage occur secondary to laminitis insult that was either not appropriately addressed in a timely fashion or so severe that any mechanics would not have changed things sucha as in severe sinker cases. Lobo did not receive the needed tenotomy until 6 wks post laminitis and the initial insult was severe creating compromise at the circumflex. This is noted in the venogram obviously but also in the shape of the tip of the coffin bone. You can see flipped up circumflex starting to remodel around the apex.


 Initially placed in Rocker Rail to increase PA and removed crushed heels.
Initially placed in Rocker Rail to increase PA and removed crushed heels.
Note the still compromised solar vascular supply with lack of papillae but nice remodelling of the circumflex artery.







Points to remember: Evaluation of the vascular supply is paramount to determine success of the device you are applying. Success should not only be measured by comfort of the patient but I cannot claim success without even toe to heel growth and addition of 7-10mm of sole depth every 30 days. If this is not happening one must rethink their approach. Note we did not have a natural increase in Palmar angle we created is due to upright pasterns. The upright pasterns can be secondary to continued low grade bone pain or even some heel pain. Achieving better digital alignment allows load be directed through the middle of the foot in the direction that the first phalanx is pointing.
Lobo is now getting 4-6 hours of paddock turnout after five months of stall confinement with the first three in firm wraps over tenotomy site to prevent excessive scarring and a tenotomy rail shoe to prevent toe from flipping up or undue strain on tenotomy site in soft stall bedding.
Please comment, email (iepvs11@gmail.com) or call (9182351529) if you have any questions.
Thursday, December 29, 2011
Images from the October Podiatry clinic with Dr. Ric Redden, DVM
I hope all are having a great holiday season. Kellee and I wish all of you the best in the new year. We are looking forward to new podiatry cases and meeting new clients.
I am finally getting some time to post some images from the Redden clinic we hosted here in Tulsa Ok back in October. We had a great time and had some good cases to work on. Two cases I have continued to follow with radiographs and one with venograms. Dolly the mild laminitis case we used as a venogram demonstration case I plan to post separately as a single case report after our next shoeing and venogram next month. She was an interesting case and I have lots of images. She is doing well and growing nice foot mass.
I can't thank Dr. Redden enough for spending his time with us in Tulsa. Anyone that may be interested in attending future clinics in Tulsa please email us a iepvs11@gmail.com.
I will also be posting an update to Lobo the laminitis case with recent radiographs, shoeing approach and venograms.
Please look back in the archives to view many other cases and images. I will be posting two more laminitis cases soon as well.
First case is a chronic navicular with rotational and varus limb deformities. Goal is to increase tendon surface angle, Palmar angle and reduce digital breakover.


Below: Quarter race horse that goes off after 150 yards or so and quits running. 4yrs old and has moderate navicular changes already. Placed in Rockered Race shoe from NANRIC to increase TSA and PA. This will unload DDF/nav bone engagement and small osteophyte at dorsal aspect of coffing joint.







 The next case with thin soles and crushed heels. Poor quality foot mass. Placed in a rockered full rocker from NANRIC to increase PA unload DDF and increase circulation and unload solar corium. Better digital alignment is also another benefit of the rocker shoe application.
The next case with thin soles and crushed heels. Poor quality foot mass. Placed in a rockered full rocker from NANRIC to increase PA unload DDF and increase circulation and unload solar corium. Better digital alignment is also another benefit of the rocker shoe application.



 This case was a grade 2 club. The owner reports the horse had a check ligament desmotomy at 18 months and is now 2 years. Note the Large bone angle in the Left Front and the boney changes that accompany the club foot forces, bump on dorsal aspect of coffin bone about halfway down and remodeled apex. All load induced lesions. This case is a barrel horse prospect and not actively training that much. Dr. Redden decided to maintian in four point trim for now and is needed to help maintain good foot mass while in performance a rockered flat steel shoe and or a full rocker.
This case was a grade 2 club. The owner reports the horse had a check ligament desmotomy at 18 months and is now 2 years. Note the Large bone angle in the Left Front and the boney changes that accompany the club foot forces, bump on dorsal aspect of coffin bone about halfway down and remodeled apex. All load induced lesions. This case is a barrel horse prospect and not actively training that much. Dr. Redden decided to maintian in four point trim for now and is needed to help maintain good foot mass while in performance a rockered flat steel shoe and or a full rocker.


I am finally getting some time to post some images from the Redden clinic we hosted here in Tulsa Ok back in October. We had a great time and had some good cases to work on. Two cases I have continued to follow with radiographs and one with venograms. Dolly the mild laminitis case we used as a venogram demonstration case I plan to post separately as a single case report after our next shoeing and venogram next month. She was an interesting case and I have lots of images. She is doing well and growing nice foot mass.
I can't thank Dr. Redden enough for spending his time with us in Tulsa. Anyone that may be interested in attending future clinics in Tulsa please email us a iepvs11@gmail.com.
I will also be posting an update to Lobo the laminitis case with recent radiographs, shoeing approach and venograms.
Please look back in the archives to view many other cases and images. I will be posting two more laminitis cases soon as well.
First case is a chronic navicular with rotational and varus limb deformities. Goal is to increase tendon surface angle, Palmar angle and reduce digital breakover.




Below: Quarter race horse that goes off after 150 yards or so and quits running. 4yrs old and has moderate navicular changes already. Placed in Rockered Race shoe from NANRIC to increase TSA and PA. This will unload DDF/nav bone engagement and small osteophyte at dorsal aspect of coffing joint.




Next Case: Older teenage trail and lesson horse. He has been plagued with Navicular disease and is 2/5 lame on left front. Immediate improvement is noted and absolutely no head bobbing at next reset. The first three images are from the day of the clinic and the last two are pre shoeing radiographs from the reset. I misplaced the day of the clinic rads for this case.


 |
| This is is post trim with application of barium paste to accentuate the trim performed by Dr. Redden. |








 |
| Post 4 point trim. Note improved digital breakover created by the slight bevel in toe |
Thursday, November 24, 2011
Update on Severe White line disease case
It has been a while since my last post. I am writing this as we are driving down the road headed to visit family on Thanksgiving Day. We had a great clinic in October with Dr. Ric Redden. I plan to post images from the clinic. We had an interesting mild laminitis case in which we performed venograms the day of the clinic and we did follow up venograms about 2 weeks later.
The case below is one we have been working with for several months and it is coming along very well. We had our most dramatic increase in sole depth this last cycle and we now are very close to what I would consider a normal sole depth for this size of horse. The fungal invasion noted by defects in the hoof wall on radiographs and visual inspection is no longer present. We reset the rocker rails with positive pressure frog bar and plan to have the next visit in conjunction with regular farrier and turn it back over for 2-3 cycles.
Please look back at previous post for comparative photos and radiographs.





 We reset the rockers using nails against the hoof wall and superfast adhesive to attach nails to hoof wall. One roll of 2 inch casting tape was then applied over that.
We reset the rockers using nails against the hoof wall and superfast adhesive to attach nails to hoof wall. One roll of 2 inch casting tape was then applied over that.
HAPPY THANKSGIVING!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
The case below is one we have been working with for several months and it is coming along very well. We had our most dramatic increase in sole depth this last cycle and we now are very close to what I would consider a normal sole depth for this size of horse. The fungal invasion noted by defects in the hoof wall on radiographs and visual inspection is no longer present. We reset the rocker rails with positive pressure frog bar and plan to have the next visit in conjunction with regular farrier and turn it back over for 2-3 cycles.
Please look back at previous post for comparative photos and radiographs.






HAPPY THANKSGIVING!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
Tuesday, September 20, 2011
White line disease Cases
Hello Everyone, I am attempting to redesign my blog. I am trying to design to have a page for each disease process of the equine hoof. This is an update to the severe white line disease case I have been working on for the last few months. Considerable progress has been made noted by good hoof wall growth free of fungal invasion and good sole depth recovery. The foot has regenerated and is looking more like a foot should. One area on the lateral (outside) toe of the right front that has not responded and has invaded the new growth. During this visit I completely removed all horn affected and this is the only spot that I needed to remove part of the new growth.








I was able to get a couple of nails in the heel region but mostly nails are glued to the inner layers of horn wall. Please look back at the previous months post's to see pictures and radiographs. After the pictures I wrapped a 3" casting tape for added security but removed any glue or cast material over the Lateral toe site so the owner could clean and treat with keratex hoof hardener, but mostly keep it open to the air.








Subscribe to:
Posts (Atom)