Theory of Two Loads
I have
struggled with what forces are involved in the hoof and how they changed with
different palmar angles and varying degrees of deep digital flexor tension
(DDF). So to aid in my understanding I consider two extreme examples to help
describe my simplified idea of two major loads within the hoof capsule. First I will describe tendon load (TL) and
the extreme example to be used is a high grade club. Next we will discuss bone load (BL) or ram
load with the extreme example of a post ddf tenotomy laminitis case.
I think we can all agree that there is a
significant pull from the DDF in club foot cases. Lets consider the action of the DDF. As weight is applied to the limb or the DDF
muscle contracts the pulling force is
transferred to the coffin bone via the semilunar crest at the DDF tendon
insertion. This pulls the coffin bone
around its articulation with the distal end of the second phanlanx (P2) and the
DDF tendon also is pressed against the flexor surface of the navicular bone. Extraction forces are apparent at the
horn-lamellar interdigitation and compression forces on the solar corium
directly beneath the apex of the coffin bone.
Club feet are affected by a shortened musculotendonous unit via
increased neurologic stimulation of the flexor muscle. This tranfers load to the apex of the coffin
bone and the horn-lamellar interface at the toe. So for simplicity sake consider two lengths
of rope both attached above carpus and at the semilunar crest of coffin
bone. The shorter length will transfer
more load to the apex than the longer when weight is applied to the limb.

Figure 1 short rope/high pa/club
Figure
2 Longer Rope/low pa/slam dunk
These forces and the changes
implied are noted on radiograph's of club feet, as a remodeled tip of coffin
bone, a small bump midway down on the face of P3 and often smaller,and a less
dense navicular bone. These changes
follow Wolfes law of bone remodels along lines of tension and compression. Now consider the external characteristics of
this extreme example: Atrophied frog,
deep central sulcus, wider growth rings at heel than toe, bulging or flat sole
at and around apex of frog. These
characteristics are created by the excessive DDF tension which allows for an
unbalanced load distribution between tendon load and bone load. This excessive TL prevents loading and
stimulation of the palmar portion of the hoof and leaves the frog and heel
suspended in the air.
.
Figure 3 bone remodeling on tip of coffin bone
The
second load to consider is bone or ram load (BL). This is the weight that is transferred
through the bony column directly to the ground.
If no DDF was present then all load is distributed through this manner
and forces are increased in the heel region.
Consider the case of a post deep digital flexor tenotomy when all TL has
been negated due to severing of the DDF tendon. All weight and forces are concentrated in the heel region
and has more of a table leg distribution of forces. I feel that many of the crushed heel, low to
negative palmar angle hooves have a
similar situation. Just as the club foot is born with shortened musculotendinous
unit the low Palmar angle/crushed heel or slam dunk foot may have a longer than
ideal musculotendinous unit allowing a greater bone load that will allow more
weight or load through the bony column to the palmar/plantar aspect. I think it is possible to create a negative
palmar angle and crushed heels with poor mechanics in many of our everyday
shoeing practice that could possibly take a normal healthy foot with good sole
depth and palmar angle to thin soles and negative palmar angle, however many
are destined for that path from a very early age due to conformation. It is impossible to take a club foot
caused by shortened musculotendinous unit and create a negative palmar angle
and the same may be true for the slam dunk foot as many will revert back to
crushed and under run heels once orthotic devices have been applied to increase
hoof quality, sole depth and aid in treatment of lameness.
Consider a
heel sore horse that is landing toe first, this is evidence to me that the
horse can use the tendon to transfer load to the front of the foot to unload
the painful buttress, digital cushion and many related soft tissue
structures. Many horses compensate quite
well by transferring load to the front of the foot via DDF with initial heel
soreness but it is not long until the extra workload by the tendon creates inflammation
within the tendon itself and many of soft tissues and ligaments associated with
the palmar/plantar aspect and fatiguing the flexor muscle group. This is when
a trip to the vet usually occurs as they are now unable to effectively transfer
load to a non painful region and show obvious signs of lameness. The increased load transferred to the front
by the toe first landing and often long digital breakover in these cases
decreases blood supply to vital growth centers and adds to the further compromise
of hoof and sole quantity and quality.
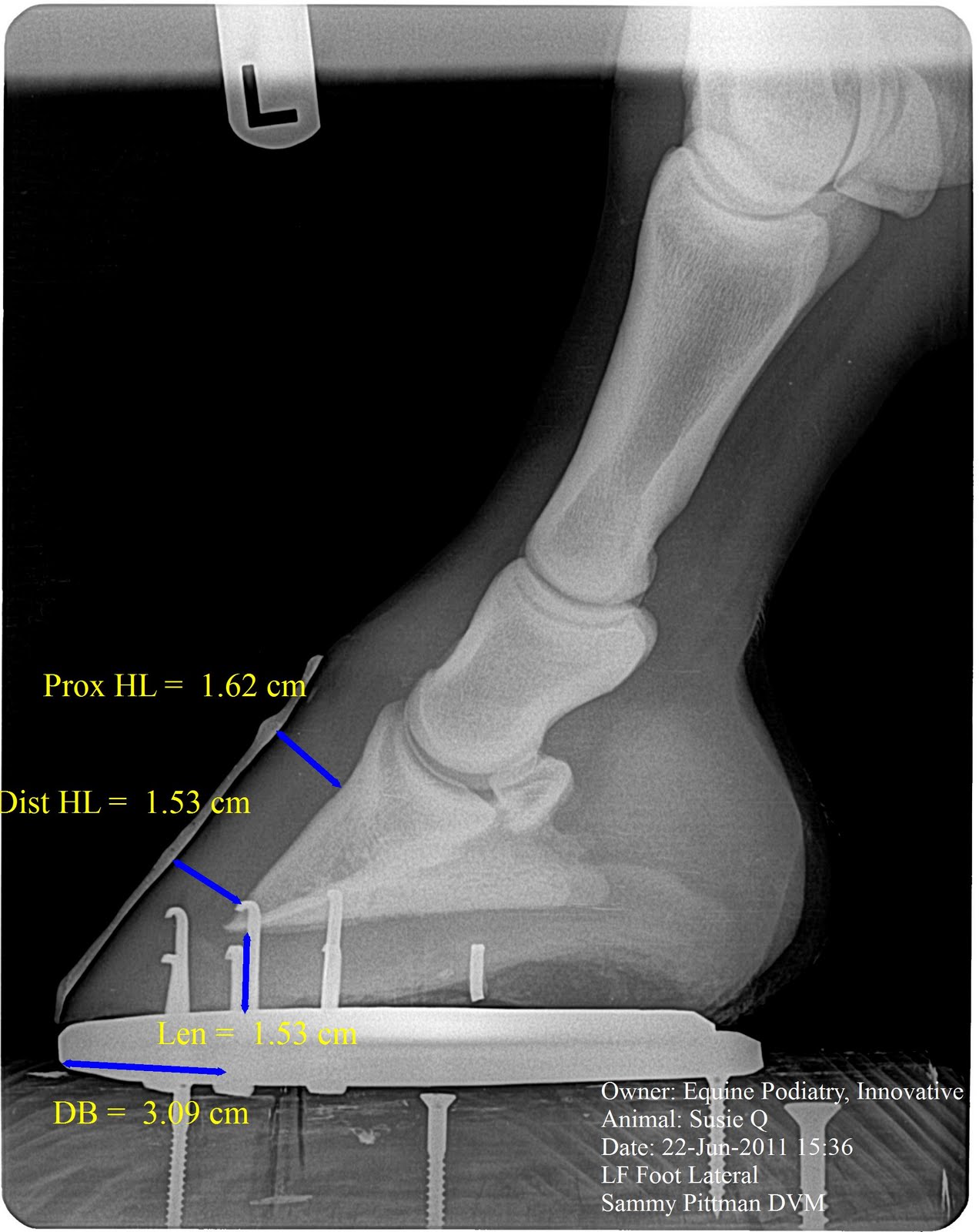
Radiographs would show very thin soles below wings of coffin bone, low
to negative palmar angle, a very low tendon surface angle, as scallop of bone
remodeling in palmar/plantar aspect of solar margin of coffin bone and upright
pasterns. External characteristics noted
are: Wider growth rings at toe than
heel, flat and thin soles, 2-3 sets of nail holes, wide robust frog, and under
run heels.



Figure 4Low Pa bone remodeling/low
ddft tension
For
further understanding let us consider treatment of these two scenarios and why
they are successful l in
increasing soundness and quality of hoof mass.
For the club foot syndrome, lower grades that are not surgical
candidates, increasing palmar angle and lengthening the heel base will allow
more BL and less TL. Decreasing the TL
will decrease the amount of load being transferred to the toe and allow more
bone or ram load to push into the heels.
The easiest and most successful approach I have found, is using rocker
shoe mechanics. The heels are trimmed to
the widest part of the frog parallel to the wings of the coffin bone and toe is
trimmed perpendicular to the frog axis at a low rocker toe style angle.
Figure 5 Grade 3 club
Figure 6 Grade 3 club with Rocker Rail
The trim will vary based on such parameters as
palmar angle, sole depth and digital breakover but the basic approach will stay
the same. The next step is to determine
what shoe to shape to fit our specific needs.
In general low grade clubs will do fine in a rockered flat shoe as
higher grade clubs may require starting with a wedged shoe that has greater
mechanical potential. Consider a flat
shoe that is rockered can alter pa 2-4 degrees and a 5 degree rail shoe is
starting with 5 degrees, so any added rocker will increase potential to alter
palmar angle. So the question to be
answered is how much PA increase do I need to create less tendon load and more
bone load? Low grade clubs require less
than higher grades. This approach will
allow more ram or bone load, more heel loading that will result in less atrophy
of the frog, decreasing depth of the central sulcus, increased sole depth below
the tip of coffin bone and more even toe to heel growth patterns. With less TL comes less H/L zone extraction
force and less solar corium compression.
Now consider a case of acute
lamintis with extensive H/L detachment and venogram shows decreased perfusion
at the coronary waterfall, compromised vasculature down face of the coffin
bone, tip of coffin bone has displaced 3
mm below the circumflex artery, and terminal papillae are horizontal versus
being in normal orientation with the face of p3. This gives us a picture of severely
compromised dorsal portion, including the horn-lamellar attachment and solar
corium below the tip of coffin bone. A
DDF tenotomy may be indicated in many cases such as this. This will completely
unload the forces of the DDF and allow all weight to be transferred down
through the bony column into the palmar/plantar region of the foot and unloading
much of the compromised areas in dorsal aspect. This can be shown by post tenotomy
radiographs and venograms. This
release and increased load now through the bony column to heels will often push
the coffin bone up closer to its original placement prior to laminitis episode
and displacement and radiographs will show measurable decrease in distal h/l
zone and increase in sole depth just from the unloading that occurs from
complete release of DDF.

Figure 7 laminitis with rotation
Figure 8 Post tendon cutting and derotation shoeing
Figure 9Acute laminitis venogram
In the above drawings (Figure 7 and 8) shows
the pull of the tendon with detached bone to horn attachments and a post
tenotomy with derotational shoeing.
Without a healthy lamellar attachment there is no antagonistic force to
counteract the pull of the ddft (TL) and the coffin bone rotates around its
articulation compressing solar corium at the tip of the coffin bone. Figure 9 shows an acute laminitis case in
which the bone is compressing the blood supply at the tip of coffin bone due to
lamellar detachment. You can see the tip
of coffin bone below the circumflex artery.
This area is heavily loaded secondary to the TL and loss of the bone to
horn attachment. The image on the right
is of the same horse 2 weeks after derotational shoeing and deep digital flexor
tenotomy. The tenotomy negates all TL
and its forces applied to the damaged areas (lamellar zone, sole under tip of
p3) and heavily loads the palmar/plantar aspect of the hoof through BL only. Note the restructuring of the blood vessels
under and around the tip of the coffin bone in this short 2 week period.
I have always considered that
anytime we raise the palmar angle via wedges or rocker shoe mechanics that we
increased the load on the heels but it really wasn't clear why until
considering these two loads. These
examples are two extreme versions and most feet will fall somewhere in between.
When a healthy balance between TL and BL
exist we find good feet that are easy to
maintain with adequate sole depth and a positive palmar angle but when loads
sway more to one side of spectrum to overloaded portions become unhealthy and
need our assistance in balancing the load via a well designed protocol based on
and monitored by serial podiatry style radiographs and venograms.













































{kind=link}